
Originally published on the Legal Glass Substack and republished with permission.
On December 5, 2025, the CDC’s Advisory Committee on Immunization Practices (ACIP) voted 8–3 to move the HepB birth dose into Shared Clinical Decision-Making and to recommend beginning the series “no earlier than two months.” On paper, the shift looks modest. In reality, it marks the first meaningful breach in a system that has long treated parents not as partners in their children’s medical care but as obstacles to be managed. The vote is not yet final—acting CDC Director Jim O’Neill must still approve it—but if adopted, it will undo a deeply questionable practice: vaccinating hours-old infants born to HepB-negative mothers not because evidence showed they were at risk, but because adults who were at risk refused the shot.
The revised recommendation merely restores the starting point to the two-month visit—where it once stood in the United States and where it remains throughout most of the developed world. Yet instead of welcoming a modest, globally aligned recalibration, the medical establishment erupted. The American Academy of Pediatrics (AAP)—which receives substantial funding from the pharmaceutical industry—claimed the ACIP recommendation “sowed fear and distrust in vaccinations.” The New York Times proclaimed a “credibility crisis.” Pharma-aligned commentators declared ACIP “ideological.” Legacy epidemiologists accused reformers of “politicizing” vaccine policy.
The irony is glaring. For decades, the same institutions now lamenting “politicization” championed school and employment mandates, eliminated exemptions, pathologized parental hesitation, and insisted that bureaucratic authority should override parental judgment. Mandates are political. Removing choice is political. Silencing dissent is political. The only reason the establishment suddenly objects to “politicization” is that—for the first time in decades—political power is no longer reinforcing their worldview.
Anyone who actually watched the two-day ACIP meeting—not the headlines, but the testimony—saw immediately why that shift threatens them. When placed in public view, the old guard’s authority depended not on evidence but on indignation, condescension, and a reflexive drive to silence critics. On one side were those intent on preserving a paternalistic, opaque, unaccountable structure. On the other were reformers insisting on transparency, rigorous data, true placebo-controlled trials, and the restoration of informed consent.
ACIP hearings have long functioned as automatic affirmations of the status quo—until now. For the first time, the public saw competing arguments presented side by side, and the difference was stark: one camp grounded in evidence and humility, the other in ego and preserving a highly profitable, but failing system.
What Happened at ACIP: Shaming, Rage, and Panic at the Loss of Control
The ACIP meeting revealed the old guard’s playbook with painful clarity. The moment inconvenient data entered the discussion, several defenders of the status quo reverted not to scientific analysis but to indignation and rehearsed talking points. Jason Goldman, MD—appearing on behalf of the American College of Physicians—chastised the committee for even entertaining debate outside the approved narrative. Joseph Hibbeln, MD, a voting ACIP member, brushed aside concerns about the lack of long-term safety data. And Cody Meissner, MD—one of ACIP’s most outspoken traditionalists—insisted there is “no evidence of harm” from the newborn HepB dose, while sidestepping the central point: there is no evidence because no one ever looked. Decades of short follow-up, non-inert placebos, and the absence of neurodevelopmental monitoring ensured that harms would remain unknowable by design.
These were not mere scientific disagreements. They were attempts to end scientific disagreement—to reassert authority by repeating institutional mantras rather than engaging with the data and urging that discussion be shut down altogether. Dr. Ray Pollak went even further, claiming Americans are not sufficiently “well-versed” in immunology to make decisions for their own children—without acknowledging that this supposed ignorance is the predictable result of a system that has spent decades withholding data, obscuring risk, and ridiculing anyone who asks to see the evidence.
In stark contrast, the reformers—Retsef Levi, Tracy Hoeg, Evelyn Griffin, Mark Blaxill, Robert Malone, and others—presented the evidence the old guard has avoided for decades: no randomized newborn trials; safety cohorts monitored for only a few days; no long-term autoimmune or neurodevelopmental assessments; documented injury patterns in VAERS, case reports, and federal courts; biologically plausible mechanisms linking aluminum adjuvants and yeast-derived antigens to inflammatory disease; and international comparisons showing the U.S. as a global outlier.
Where the reformers raised evidence, the old guard raised defenses. Where the reformers asked questions, the old guard insisted the questions themselves were illegitimate. And the public—watching in real time—saw exactly who argued from data and who argued from authority.
And this is why the stakes are so high: although CDC and ACIP recommendations are technically voluntary, they function as the regulatory backbone for state-level mandates, school-entry requirements, hospital protocols, and employment rules. In practice, what ACIP recommends often becomes what Americans are compelled to do.
Why the Universal Newborn HepB Dose Was Paternalism at Its Worst
The universal newborn dose was never rooted in infant risk. Infants born to HepB-negative mothers face essentially zero likelihood of early-childhood infection. ACIP knew this when it implemented the policy. The dose was adopted not to protect babies, but because adults at risk refused it—and because newborns could not refuse.
Internal language describing hospitals as a “reliable point of contact” reveals a mindset that prioritized bureaucratic convenience over parental autonomy. The setting guaranteed compliance: exhausted mothers were handed refusal forms implying danger, warned that Child Protective Services might be involved, or told the vaccine was required. Stories of nurses vaccinating newborns against parental wishes were not uncommon. Financial incentives—from guaranteed reimbursement to liability shields—then hardened the policy into dogma. It was never about infants; it was about preserving a system that rewarded compliance and punished dissent.
What the old guard fears now is simple: once the dose is no longer administered in the hospital—when parents are vulnerable, captive, and overwhelmed—many will decide not to accept it at the two-month visit either. They may delay it, question it, or choose to forgo it altogether. They may read about documented adverse effects, examine VAERS data showing thousands of reports of injuries and deaths, or finally feel free to educate themselves about the true risk–benefit profile rather than being pressured into compliance. In other words, the establishment fears parents exercising informed consent—because informed consent leads to individualized decisions that do not always align with their recommendations.
Aaron Siri Challenges the Entire Childhood Vaccine Schedule
If the HepB vote rattled the old guard, what followed shook the entire foundation. After the vote, attorney Aaron Siri delivered a presentation that challenged the scientific underpinnings of the entire childhood vaccine schedule. He laid out what most parents have never been told: that none of the vaccines on the schedule were tested against inert placebos; that manufacturers used other vaccines, adjuvants, or non-inert substances as “controls”; that safety monitoring often lasted only days; and that the 1986 National Childhood Vaccine Injury Act eliminated market incentives to improve safety by shielding manufacturers from liability altogether.
It is telling that Paul Offit and Peter Hotez—vaccine developers and two of the loudest critics of ACIP reformers—were both invited to appear alongside Siri and declined to participate. They were eager to attack from television studios, but unwilling to engage in a forum where evidence could be scrutinized and questions answered.
Siri closed with the truth the establishment avoids—quoted here in full because every word matters:
“If you want to increase vaccine confidence, you must depoliticize vaccines. And the way to depoliticize vaccines is to end mandates. Mandates make vaccines political. When you take away someone’s rights, you turn a medical question into a political and legal one.”
In a single sequence, he revealed why the old guard depends on censorship, why questions are treated as threats, and why transparency triggers panic: mandates cannot coexist with informed consent. A system that requires universal compliance cannot withstand honest scrutiny, because informed people may choose to refuse.
That is why the backlash was—and remains—so visceral.
ACIP member Cody Meissner, visibly shaken, accused Siri of presenting “a terrible distortion of all the facts,” and invoked Offit—whose long-standing financial conflicts should have disqualified him from ACIP or the Vaccines and Related Biological Products Advisory Committee (VRBPAC)—as though the mere citation of his name could resolve the argument. Meissner then praised the ballooning U.S. childhood schedule—the highest in total vaccines and total doses among developed countries—as “a phenomenal accomplishment,” described certain vaccines as “wonderful and remarkable,” dismissed the concerns raised as “very rare, ill-defined side effects,” and concluded:
“For you to come here and make these absolutely outrageous statements about safety…I think…it’s a big disappointment to me, and I don’t think you should have been invited.”
It was the reaction of someone watching the foundations of his life’s work being challenged in real time.
Siri’s reply was measured and far more devastating. Meissner sees the world through the lens of an infectious-disease physician, Siri said—someone trained to focus on harms caused by pathogens, not the harms that can result from the interventions themselves. He noted that he had already debated Offit publicly on Twitter and invited the committee to review that exchange and its citations, underscoring that nothing Meissner invoked was unexamined or undisputed. Siri, by contrast, sees the world through the lives of the vaccine-injured—“real harms, real people who are hurting.”
And then he delivered the line that captured the moral turning point of the meeting:
“Your failure to acknowledge them will be your precious vaccine program’s undoing.”
COVID Changed Everything—We Are Done Being Managed
Before 2020, many parents accepted public health recommendations at face value and complied with a steadily expanding vaccine schedule. COVID ended that era. During the pandemic, families watched the same agencies that insisted newborns needed HepB on day one push mandates for a platform never before used in healthy populations; deny myocarditis risks in adolescent boys until the evidence became impossible to hide; misrepresent transmission; attack credentialed scientists who raised valid concerns; coordinate censorship; rewrite definitions to drive uptake; and dismiss adverse-event signals that later proved tragically real.
Parents learned, unmistakably, that when political expediency collides with scientific uncertainty, the system protects the narrative—not the public. COVID didn’t create mistrust; it revealed that trust had been profoundly misplaced. And parents who lived through that will never again accept “because we say so” as a medical argument.
This is the context in which the ACIP HepB vote arrives. It is not an endpoint but the beginning of a reckoning—a recognition that a system built on secrecy, coercion, and unexamined dogma cannot survive in a world where the public finally demands evidence. The establishment’s furious reaction makes clear how destabilizing that shift is. Their authority depended on parents never looking behind the curtain. That era is over.
Parents were never too “uninformed” for meaningful consent; they were denied it by institutions afraid of what informed parents might conclude. And after COVID—after seeing exactly how far those institutions will go to maintain control—the country is no longer willing to defer blindly or absorb the consequences in silence.
The age of medical paternalism is ending.
It cannot happen soon enough.
Rita is a medical freedom attorney and former law school professor who now writes on a variety of medical freedom issues. A former FNF board member, Rita was also part of the legal team at FLTJ, the firm that represented Free Now Foundation in lawsuits against K-12 Covid mandates and prolonged states of emergency. You can follow more of Rita’s work at: https://legalglass.substack.com/



I heard California will will ignore ACIP recommendations and continue with the ‘old’ plan. Therefore, any state should be held liable for injuries for vaccines!
Your headline says “except in California“ but the article doesn’t address California at all. I’m anxious to hear what you meant!
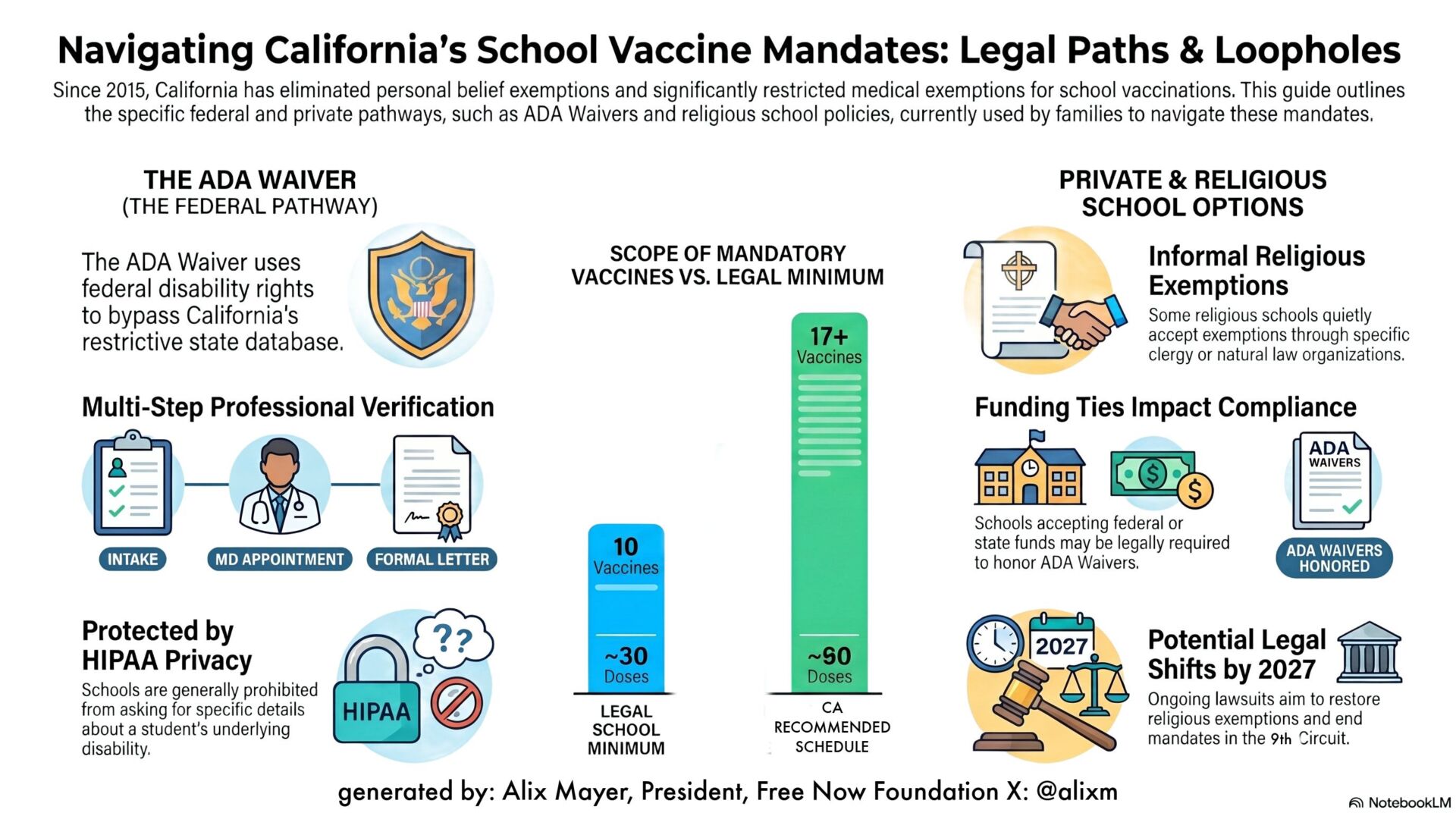
You are right – the article could have been more clear on that. When Newsom signed AB144 into law, he pegged the California schedule to CDC’s January 2025 schedule. That means the CA schedule includes COVID shots, Hep B birth dose, and MMR-V as “recommended.” Meanwhile, ACIP has advised CDC to move COVID shots down from “recommended” to a lower level: doctor-patient decision-making, and not recommend the MMR-V due to higher risk of seizures. CDC adopted those recommendations, but California does not recognize that. Last ACIP meeting, the members voted 8-3 to not administer a birth dose of Hep B vaccine except in the case of a Hep B positive mother. ACIP also recommended the Hep B shot be moved down from recommended to doctor-patient decision-making. CDC is expected to adopt that recommendation. California will not change its schedule based on ACIP or CDC changes. Only California’s public health department will make changes to the California schedule.
Wonderful commentary.
I would like to see a follow up article about how this ACIP vote will apply to CA. CA has decided to keep the old vaccine schedule dated 1/2025. What happens to CA once the Hep B shot is no longer federally recommended? Does the lack of CDC recommendation change doctor’s liability? What will informed consent to the shot in CA look like?
How can we influence and possibly get rid of the West Coast Health Alliance? Can it be challenged in court?
I am anticipating that ACIP will change the entire childhood vaccine schedule. All of the above questions would apply to that scenario too.
Thanks for your questions, Mary! When Newsom signed AB144 into law, he pegged the California schedule to CDC’s January 2025 schedule. That means the CA schedule includes COVID shots, Hep B birth dose, and MMR-V as “recommended.” Meanwhile, ACIP has advised CDC to move COVID shots down from “recommended” to a lower level: doctor-patient decision-making, and not recommend the MMR-V due to higher risk of seizures. CDC adopted those recommendations, but California does not recognize that. Last ACIP meeting, the members voted 8-3 to not administer a birth dose of Hep B vaccine except in the case of a Hep B positive mother. ACIP also recommended the Hep B shot be moved down from recommended to doctor-patient decision-making. CDC is expected to adopt that recommendation. California will not change its schedule based on ACIP or CDC changes. Only California’s public health department will make changes to the California schedule.
Liability for any injury or omission has been waived for: prescribers, dispensers, orderers, furnishers, or administrators of vaccines on the CA-only schedule.
We are working with our attorneys to find a way to challenge the law enacted by AB144. Since the Constitution is silent on medical freedom, the powers rest with the States. The best thing people can do now is sign our petition on our home page to notify 8 public officials of the problem here. In 2026 we will use those signatures and formally request help from the federal officials and their agencies. freenowfoundation.org