
Originally published on The Legal Glass Substack and republished with permission
This week, Governor Gavin Newsom announced yet another grand-sounding public-health initiative—PHNIX, the Public Health Network Innovation Exchange—pitched as “innovation,” modernization, and scientific leadership in response to what state officials describe as a federal retreat from “science.”
But PHNIX is not a neutral upgrade. And it is not reform.
It is the next phase of a long-running project: the construction of a centralized public-health enforcement system—powered by technology, data aggregation, and public-private funding—designed to condition Californians’ ability to live, work, attend school, and receive benefits on compliance with state-approved medical decisions.
Newsom’s first move makes that clear: who he chose to run it.
To helm PHNIX, Newsom selected Susan Monarez and Debra Houry, former senior CDC officials closely associated with the leadership culture that presided over—and helped normalize—the coercive COVID response that shattered public trust. Monarez, in particular, comes from a health-security background centered on surveillance-oriented public health rather than clinical care—an important clue to the kind of system PHNIX is designed to become.
This is not simply resistance to reform. It is an explicit signal that California’s leadership remains committed to centralized governance of medical behavior—and comfortable importing intelligence-style surveillance frameworks into civilian public health.
California is not turning the page on pandemic governance. It is rewarding and re-recruiting its architects—and hardening their authority into permanent infrastructure.
PHNIX is not reform. It is the institutionalization of medical control.
PHNIX: A Parallel System—Built Without Consent
According to the Governor’s office, PHNIX will focus on technology development, information infrastructure, and new funding frameworks. But the initiative’s structure and stated purpose reveal something more consequential: it is designed to operate as a state-level counterweight to federal public-health reform, not as a technical supplement to existing systems.
That framing is inherently political—and deeply divisive.
PHNIX is being launched not because California voters demanded a parallel system, but because state leaders are rejecting the current federal reform agenda—an agenda that reflects both a democratic election outcome and widespread public dissatisfaction with COVID-era public health. In doing so, California is effectively telling millions of residents who support reform, including many Democrats, that their views will be overridden by a state-run counterregime.
PHNIX is not replacing the California Department of Public Health. It sits alongside it, functioning as a centralized hub supplying the technological, data, and financial architecture that will shape public-health decisions, while CDPH retains regulatory authority. The result is expanded reach with blurred accountability: a system designed to influence how medical policy is made and enforced without clear lines of responsibility or democratic oversight.
What the state has not explained is just as revealing.
Officials have not disclosed what data PHNIX will collect, whether it will include individual medical or behavioral information, who will control access, or how long data will be retained. They have not identified which private entities—technology firms, biotech companies, analytics vendors, or financiers—will participate. Nor have they explained how PHNIX will be funded, either through public appropriations or private contributions, or what safeguards—if any—would limit funders’ influence over policy.
That opacity matters. Californians may soon find themselves subject to vaccination policies and enforcement mechanisms designed and sustained by unelected private interests operating through a state-sanctioned structure voters never approved and cannot meaningfully oversee.
During COVID, appeals to “efficiency” and a purportedly “science-driven response” were used to justify centralized control, surveillance tools, vaccine passports, and the erosion of informed consent. PHNIX revives that language while offering even fewer specifics.
Absent clear limits, transparency, and democratic accountability, PHNIX does not represent modernization. It represents the construction of a parallel system of power—deliberately insulated from federal reform and public dissent.
Why Monarez and Houry Signal Escalation, Not Reform
The leadership chosen to run PHNIX makes its trajectory unmistakable.
Monarez’s background is particularly revealing. Her career is rooted not in community-based medicine or patient-centered care, but in health technology, advanced analytics, artificial intelligence, and national-security–adjacent public health programs. She has worked in and alongside agencies focused on population-level monitoring, rapid deployment of biomedical countermeasures, and technology-driven governance systems used to manage behavior at scale.
This reflects the Biomedical Advanced Research and Development Authority (BARDA) and Advanced Research Projects Agency (ARPA) model of public health—defined by centralized authority, emergency logic, tight coupling with private contractors, and faith in technological solutions to complex social and medical problems.
Her brief tenure as CDC Director ended amid conflict with reform-oriented leadership. After her removal, Monarez requested to testify before the Senate—not to reflect on institutional failures, but to challenge the reform agenda itself. When questioned about pediatric COVID vaccination, she offered evasive, qualified answers, declining to engage directly with emerging evidence or acknowledge scientific uncertainty. The performance was widely interpreted not as whistleblowing, but as political positioning—a defense of the pre-reform status quo and the managerial expert class that governed during the pandemic.
Her record does not suggest openness to public skepticism, democratic correction, or humility after failure. It suggests a commitment to rule by expert systems—enforced through data, technology, and centralized control.
Debra Houry reinforces this pattern. Although not the public face of pandemic policy, she was embedded in a leadership structure that defended prolonged school closures long after evidence of harm mounted, supported sweeping mandates, and tolerated censorship of dissenting physicians and scientists.
Reinstalling this leadership class does not signal reflection or course correction. It signals escalation.
Follow the Money
PHNIX’s emphasis on public-private “funding frameworks” should raise alarms on its own. In public health, funding is never neutral. It determines which questions may be asked, which policies are treated as non-negotiable, and whose interests shape outcomes.
During COVID, public health authority fused with private philanthropic, corporate, and technology power. Those public-private partnerships shaped policy behind closed doors, collapsed informed consent, eroded data privacy, and turned access to work, education, and public life into leverage. Entire sectors were devastated while a narrow class of companies—particularly in technology, biotech, and digital services—prospered.
California was not a bystander. The state experienced pandemic-era funding scandals, opaque contracts, and aggressive public-private collaborations that enriched vendors while offering little transparency to the public footing the bill. PHNIX proposes to deepen—not correct—that model.
By pairing centralized funding frameworks with centralized data systems, PHNIX risks formalizing the worst dynamics of the COVID era. In that environment, funding does not merely support public health—it creates incentives for surveillance, coercion, and perpetual intervention.
Power without consent is not medicine. It is management.
California’s Enforcement Ecosystem Is Already in Place
PHNIX does not exist in isolation. It fits neatly into a broader system California has been constructing for years—one that increasingly replaces individual medical judgment with centralized databases and administrative enforcement.
The passage of AB 144 this year dramatically expanded state control over vaccination policy, allowing California to issue its own recommendations apart from CDC and ACIP guidance, mandating insurance coverage, broadening who may administer vaccines, and shielding providers from liability even when federal injury-compensation systems no longer apply.
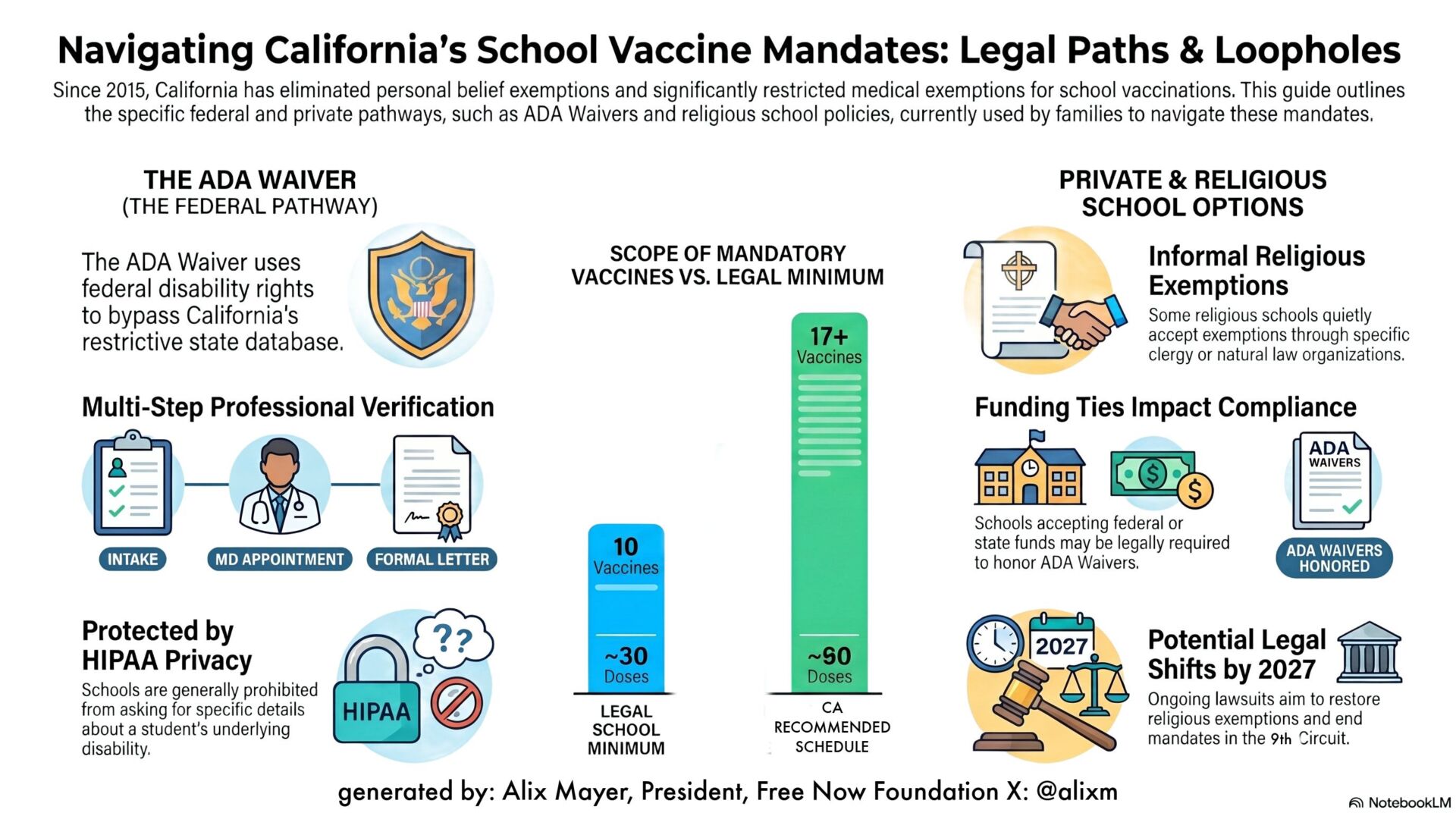
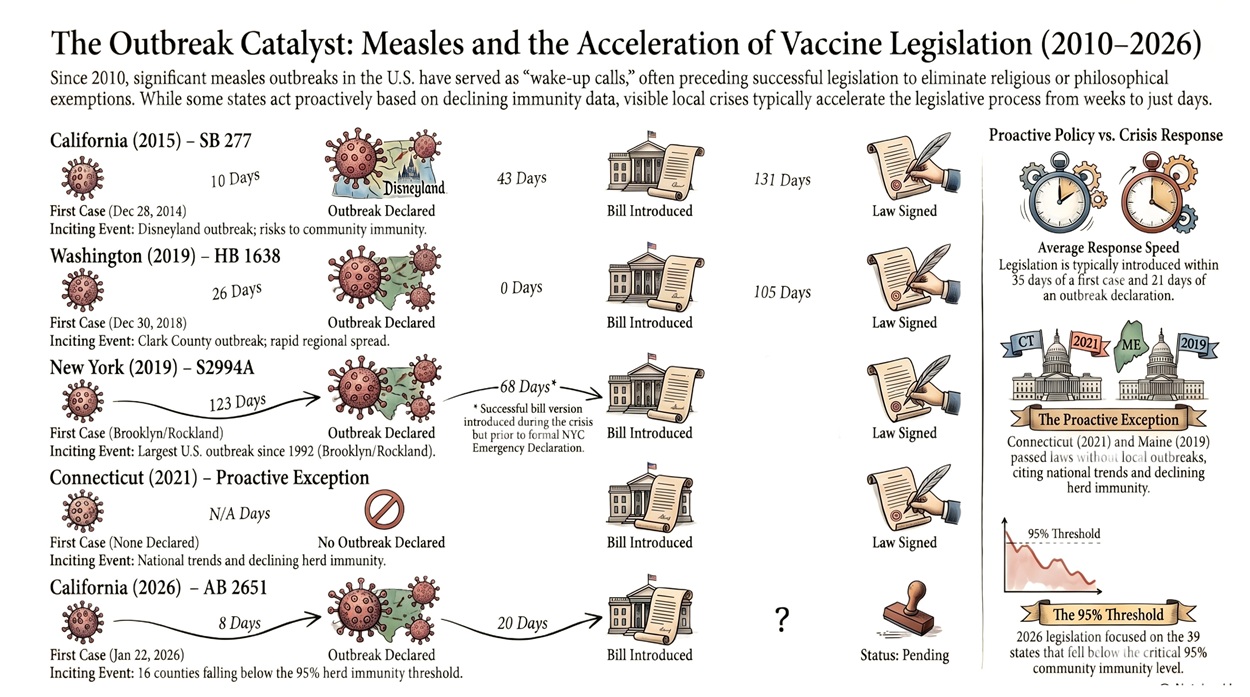
That law builds on earlier measures such as SB 277 and SB 276, which eliminated personal belief exemptions and centralized medical exemptions under state oversight, paving the way for CAIR-ME—the portal that now monitors and punitively rations medical exemptions.
Other programs extend this logic beyond schools. CalWORKs requires families seeking basic financial assistance to disclose vaccination status for young children, including those not yet school-aged, capturing medical data and conditioning access to support on participation in the system.
Layered on top are aggressive state vaccination campaigns and schedules that remain locked to prior Biden-era federal recommendations, even as national agencies reassess COVID-era excesses and childhood vaccines that never established sufficient safety data.
Taken together, the direction is clear: aggressive promotion of vaccination, centralized data collection, diminished space for dissent, expanded liability shields, and growing reliance on administrative pressure to enforce compliance. PHNIX supplies the missing infrastructure—technology and funding—to integrate and scale that system more efficiently.
At the very moment federal agencies are reassessing the failures of the COVID era, California is moving in the opposite direction—positioning its residents as the testing ground for a more aggressive and centralized regime of medical enforcement.
PHNIX Must Be Nixed
California enforced some of the longest school and business closures in the nation. It maintained mandates long after public trust collapsed. It announced—and later abandoned—a universal COVID vaccine mandate for schoolchildren, while encouraging school districts to violate existing law by imposing their own COVID shot requirements. It terminated public employees for noncompliance with a product that never stopped infection or transmission.
Now, instead of reckoning with that record, state leaders insist that federal reformers are the ones “dismantling science.” Californians are asked to believe that only the architects of the disastrous COVID response can restore trust.
But Californians are not fooled. We saw what happened. We know who was “following the science”—and who was following the money.
The phoenix is a myth of renewal—a creature that rises purified from destruction. But Newsom’s PHNIX will not rise from the ashes of the damage California’s COVID policies inflicted. It will only entrench those policies into permanent infrastructure, locking coercion, surveillance, and unaccountable power into the future of public health.
We do not need another acronym. We do not need another centralized system built without consent. What we need is restoration of informed consent, medical and data privacy, the doctor–patient relationship, and public accountability.
Before this architecture becomes permanent, PHNIX must be nixed.
Rita is a medical freedom attorney and former law school professor who now writes on a variety of medical freedom issues. A former FNF board member, Rita was also part of the legal team at FLTJ, the firm that represented Free Now Foundation in lawsuits against K-12 Covid mandates and prolonged states of emergency. You can follow more of Rita’s work at: https://legalglass.substack.com/



How do you suggest we nix it?