
This article was originally published by the California Globe on January 23, 2026. You can access the original post here. republished with permission fromThe Legal Glass Substack
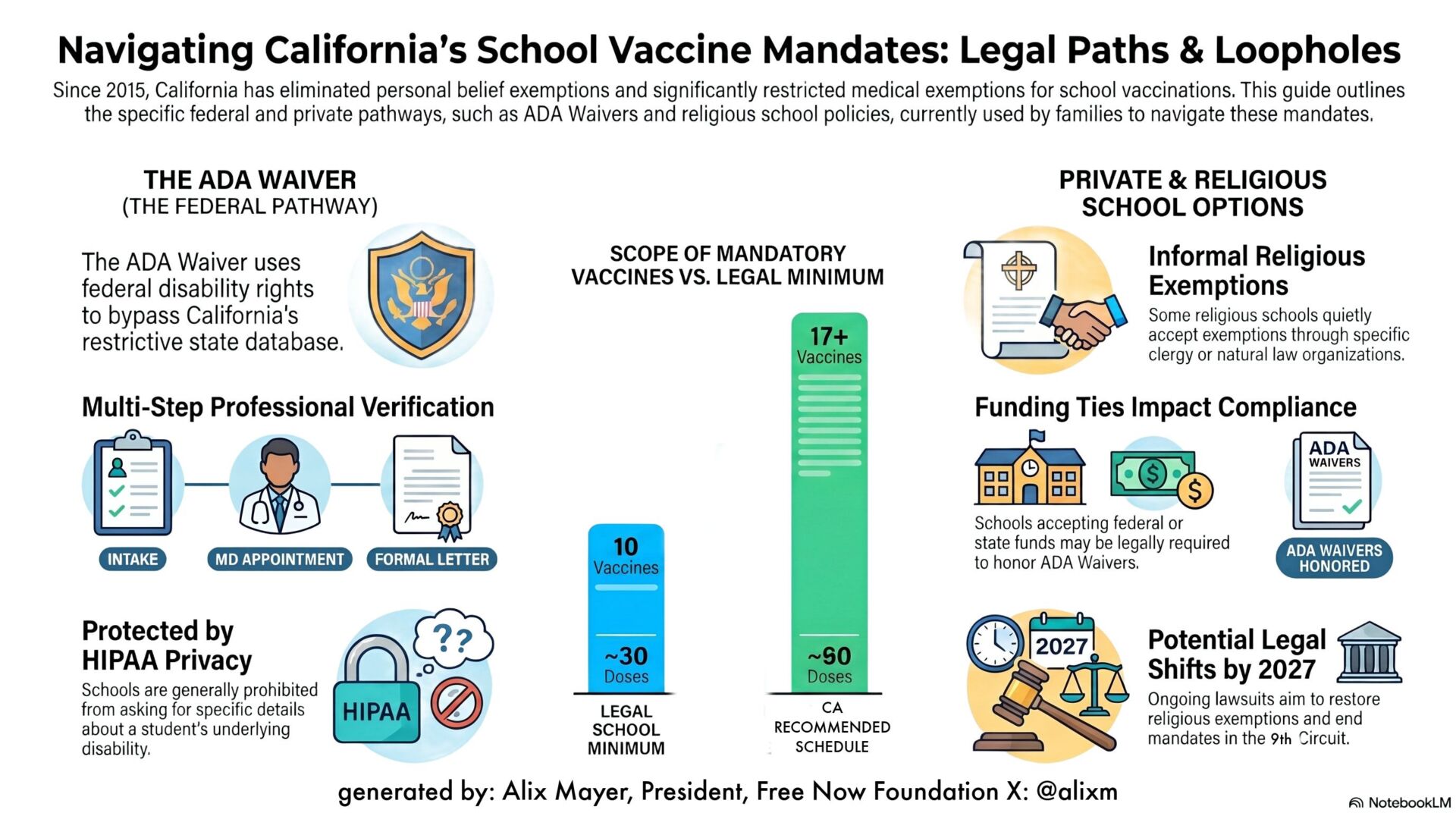
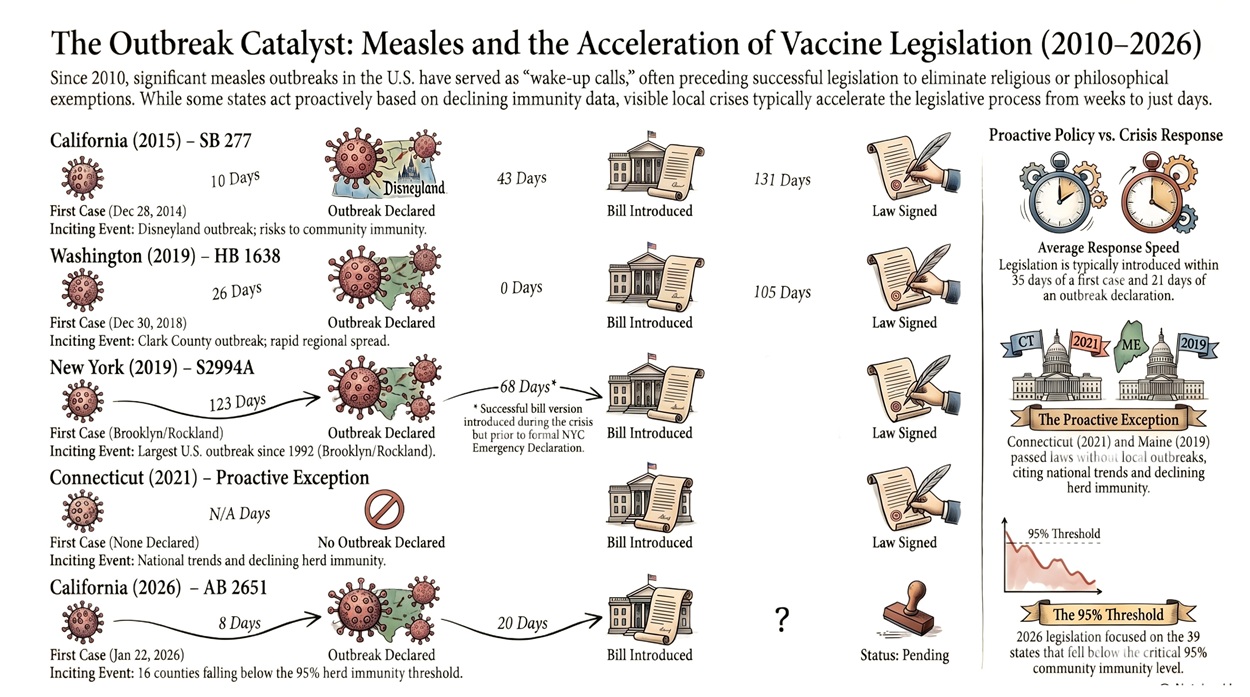
Any California parent who has tried to obtain a medical exemption in recent years—or opened a notice revoking one—has learned the same lesson: the system is rigged against them. After personal belief exemptions were eliminated in 2015 under SB 277, medical exemptions became the most viable remaining path. Today, that path is effectively closed. Doctors will not write exemptions because doing so risks their medical licenses and livelihoods.
That reality was formalized in 2019, when two bills authored by then–Senator Richard Pan—SB 276 and SB 714—radically transformed California’s vaccine policy. Lawmakers promised that medical exemptions would remain available and that physicians would retain discretion. That assurance was the lie. The legislation created a state-controlled medical-exemption registry—the California Immunization Registry–Medical Exemption (CAIR-ME)—and replaced clinical judgment with bureaucratic enforcement.
For a time, the system held because federal guidance, professional society recommendations, and California mandates largely aligned around a narrow, uniform standard of care. That alignment is now breaking down. Federal authorities are moving toward shared clinical decision-making and individualized risk assessment, while California and the American Academy of Pediatrics reject that shift. Physicians are left in a dangerous gray zone: where does the acceptable standard of care now lie?
How Medical Exemptions Were Lost in California
Under SB 276 and SB 714, all school-related medical exemptions were centralized into CAIR-ME. Exemptions must be submitted directly by a licensed physician; parents cannot file them, and schools no longer accept paper exemptions. Each exemption is vaccine-specific, permanently logged, and tied to the issuing doctor. What had once been a private medical judgment became a regulated act subject to state surveillance.
Every submitted exemption is subject to administrative review, and the statute requires heightened scrutiny when certain thresholds are met—such as low school vaccination rates or physicians issuing five or more exemptions. Beyond those triggers, CDPH retains broad discretion to review exemptions for conformity with what it considers the immunization standard of care, relying heavily on CDC, ACIP, and AAP guidance. If CDPH disagrees, it may revoke the exemption. Parents may appeal. Physicians, at this stage, may not.
Separately, CAIR-ME continuously tracks physician behavior. Doctors who issue more than five medical exemptions in a calendar year are automatically flagged, regardless of patient history or clinical justification. Once flagged, scrutiny shifts from individual exemptions to the physician’s overall practice. CDPH may then refer the physician to the Medical Board of California, where the inquiry is no longer whether a particular exemption was appropriate for a child, but whether the doctor’s pattern of judgment deviates from accepted norms.
If a physician is disciplined, the consequences extend far beyond that doctor. All medical exemptions previously written by that physician are invalidated statewide. Children relying on those exemptions must be vaccinated at the next checkpoint or attempt to find another doctor willing to write a new exemption in a system designed to make doing so professionally dangerous. One disciplinary action wipes out every exemption associated with that physician and sends a clear message to all others: independent medical judgment carries collective consequences.
The result is predictable. Faced with surveillance, automatic flagging, and retrospective enforcement, physicians stop writing medical exemptions altogether. CAIR-ME has engineered medical exemptions out of existence.
The consequences of that collapse are not abstract. They fall most heavily on children who have already been harmed by prior vaccination and are nonetheless told they must receive additional shots to attend school. They fall on families whose first child suffered a documented adverse reaction, only to be informed that there is no safe medical discretion for the next child. In these cases, the state does not dispute the injury—it simply denies its relevance. The result is a form of institutional gaslighting that forces parents to choose between their child’s health and their child’s education.
Who Decides the “Standard of Care”?
Because “standard of care” governs both exemption review and physician discipline under CAIR-ME, a basic question must be asked: who decides what that standard is?
SB 276 requires exemptions to be consistent with the “standard of medical care” or align with guidance from the CDC, ACIP, or the AAP. What the statute never does is define that standard in advance or identify a single authority empowered to declare it prospectively.
Traditionally, a medical standard of care is not a single mandated protocol. It is a range of professionally accepted approaches grounded in evidence, training, and clinical experience, within which physicians exercise individualized judgment. Guidelines inform that judgment; they do not replace it.
California’s vaccine regime operates differently. In practice, the standard of care is determined through enforcement, not law. CDPH treats federal and professional guidance as controlling benchmarks. When a physician deviates, the burden shifts to the doctor to justify that decision against an undefined immunization standard. If concerns escalate, the Medical Board decides—after the fact—whether the physician’s judgment was acceptable. Doctors learn where the boundary lies only once they are already under investigation.
The disciplinary case of California pediatrician Dr. Kenneth Stoller illustrates how this system works. Stoller’s medical license was revoked after the Medical Board concluded that his vaccine decision-making—based on individualized risk assessment and family history—fell outside the applicable standard of care. The Board rejected not only Stoller’s judgment, but also the testimony of his supporting expert, relying instead on ACIP guidance and the AAP Red Book.
The lesson was not subtle. After Stoller, most physicians did not need further warnings. Yet some continued to face investigations and disciplinary proceedings for writing exemptions that departed from prevailing immunization guidance. These cases reveal the real meaning of “physician discretion” in California: when vaccine decision-making departs from public-health consensus, even individualized, evidence-based judgment may be treated as professional misconduct.
But that framework assumes consensus exists. What happens when the federal agencies once invoked to discredit physicians like Stoller begin to reach similar conclusions?
Federal Guidance Is Narrowing—California Is Not
Federal health agencies are now moving away from blanket vaccination recommendations toward shared clinical decision-making that emphasizes individualized risk–benefit analysis. Several vaccines once treated as universally recommended—including COVID-19, influenza, meningococcal vaccines, and hepatitis B—have been moved into shared decision-making frameworks.
That shift matters. Under universal recommendations, exemptions are limited to narrow contraindications. Under shared clinical decision-making, physicians are expected to weigh exposure risk, expected benefit, and patient-specific factors. An increase in exemptions under this framework is not evidence of misconduct; it is the predictable result of practicing individualized medicine.
But even as federal agencies move toward patient autonomy and physician discretion, California public-health officials, joined by the AAP, continue to advocate for expansive mandates. Under AB 144, California further insulated its vaccine policy from changes in federal leadership by locking in prior CDC recommendations regardless of future revisions. CAIR-ME remains built for a world of uniform compliance, treating discretion as deviation even when federal guidance now requires individualized assessment.
Hepatitis B: The Pressure Point
Hepatitis B brings this conflict into sharp focus. It is not spread through casual classroom contact or everyday school interactions. Transmission occurs through blood exposure, sexual contact, or from mother to child at birth. For children born to hepatitis-B-negative mothers with no identifiable risk factors, the likelihood of contracting hepatitis B in a school setting is exceedingly low.
Under shared clinical decision-making, a physician would be expected to assess whether a child actually faces a meaningful risk of exposure. For many school-aged children, a doctor applying ordinary medical judgment could reasonably conclude that the hepatitis B vaccine is not medically necessary for school attendance and issue an exemption.
In California, that judgment carries consequences. Hepatitis B remains mandatory for school attendance. Writing more than five exemptions—no matter how carefully documented or how consistent with federal guidance—triggers automatic flagging under CAIR-ME, inviting scrutiny and potential discipline without any neutral process for physicians to defend their reasoning.
California Needs to Stop Interfering
Vaccine decisions should be made between a physician and a patient—or a parent acting on a child’s behalf—not enforced through a centralized registry designed to police medical judgment and gaslight vaccine-injured families.
As federal agencies continue to reevaluate risk–benefit tradeoffs across the childhood vaccine schedule, more vaccines may move into shared clinical decision-making frameworks. That evolution will only widen the fault line.
For now, hepatitis B may be the first vaccine to force a reckoning. It tests whether California’s assurance—that doctors remain free to exercise independent medical judgment—was ever real, or whether physicians are expected instead to function as compliance officers for a centralized public-health system.
Whether this conflict reaches the courts remains to be seen. But the more immediate test will come from physicians themselves. CAIR-ME can survive only so long as doctors accept a system that punishes them for practicing medicine. The moment enough of them refuse, the lie will no longer hold.
Rita is a medical freedom attorney and former law school professor who now writes on a variety of medical freedom issues. A former FNF board member, Rita was also part of the legal team at FLTJ, the firm that represented Free Now Foundation in lawsuits against K-12 Covid mandates and prolonged states of emergency. You can follow more of Rita’s work at: https://legalglass.substack.com/



GREAT ARTICLE! Not just physicians need to refuse to comply. Thousands of PARENTS and GRANDPARENTS and AUNTS and UNCLES and GODPARENTS need to stand up and say WE WILL NOT COMPLY.